Hi, I am Manasvi Peddineni, 3rd sem medical student.This is an online elog book to discuss our patients health data after taking their consent. This also reflects my patient centered online learning portfolio.
Case Scenario:
A 61 year old male has come to the hospital on 20th August with chief complaints of seizures and altered sensory function.
Chief Complaint:
- seizures
- altered sensorium
- brief loss of consciousness
- vomitings
History of Present Illness:
- patient was apparently asymptomatic 3 years ago, and then developed weakness, for which he was diagnosed with hypertension and was advised to take tablets TELMA - AM, but took the medication irregularly
- he was fine till 20th August when he had dinner and took the hypertension medication following which he suddenly developed brief loss of consciousness for 2 hours
- he previously came to the OPD on 3rd August with complaint of lesions on his lower limbs and during the blood tests done at that time, it was noticed that he was hyperglycemic. he was then prescribed OHA's to bring down his blood sugar levels, due to which he became hypoglycemic.
photographs of the lesions:

History of Past Illness:
- known case of hypertension since 3 years, not on regular medication
- no history of diabetes mellitus/ CAD/ asthma/ epilepsy / thyroid disorders
Personal History:
- married
- normal appetite
- mixed diet
- regular bowels
- normal micturition
- no known allergies
- occasionally consumes alcohol
Family History:
- no diabetes mellitus
- no hypertension
- no heart disease
- no stroke
- no cancer
- no tuberculosis
- no asthma
- no other hereditary diseases
Physical Examination:
- height: not taken
- weight: not taken
- BMI: not taken
- no pallor
- no icterus
- no cyanosis
- no clubbing of fingers
- no lymphadenopathy
- no edema of feet
- no malnutrition
- no dehydration
Vitals:
- BP: 110/70 mm Hg
- Pulse: 62/min
- Temperature: afebrile
- SPO2: 98% at RA liters of O2
- GRBS: 39% mg
Systemic Examination
Cardiovascular System:
- no thrills
- cardiac sounds S1 and S2 heard
- no cardiac murmurs
Respiratory System:
- no dyspnea
- no wheeze
- trachea position: central
- breath sounds: vesicular
Abdomen:
- shape: scaphoid
- no tenderness
- no palpable mass
- no bruits
- no free fluid
- hernias orifices: normal
- liver: not palpable
- spleen : not palpable
- no bowel sounds
- genitals: normal
- speculum examination : normal
- P/R examination : normal
Central Nervous System:
- conscious
- normal speech
- no neck stiffness
- no Kerning's sign
- cranial nerves: normal
- sensory : normal
- motor: normal
- reflexes: all present bilaterally
- finger nose in coordination: not seen
- knee heel in coordination: not seen
- gait: normal
Investigations:
Complete Urine Examination on 03/08/22:

Renal Function Test on 03/08/22:

Liver Function Test on 03/08/22:

Complete Blood Picture on 03/08/22:

Erythrocyte Sedimentation Rate on 03/08/22:

Random Blood Sugar on 03/08/22:

Post Prandial Blood Sugar on 04/08/22:

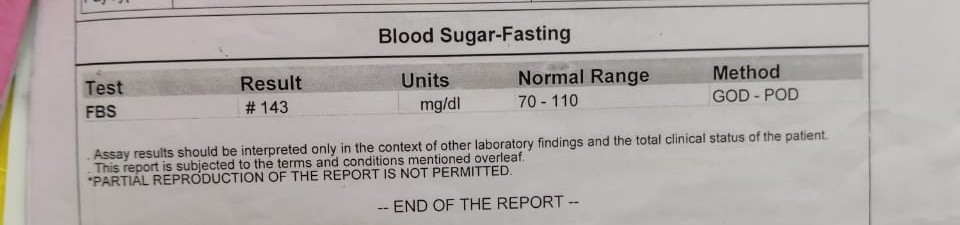
Fasting Blood Sugar on 08/08/22:
ECG:


Temperature Regulation Graph:

Ultrasound on 16/08/22:


Bacterial Culture of Pus Swab on 18/06/22:

MRI Brain on 20/08/22:

Treatment:
