Hi, I am Manasvi Peddineni, 5th sem medical student. This is an online E-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
CONSENT AND DE-IDENTIFICATION :
The patient and the attenders have been adequately informed about this documentation and privacy of the patient is being entirely conserved. No identifiers shall be revealed throughout this piece of work whatsoever.
Chief Complaint:
A 79 year old female, resident of Miryalguda, housewife by occupation, came to the OPD with the chief complaints of
- SOB since 4 days
- fever since 1month
- cough, cold since 1 month
History of Presenting Illness:
Patient was apparently asymptomatic 1 month back when she developed fever which was low grade, intermittent, not associated with chills and rigors and relieved by taking medication, associated with generalised weakness.
She also complained of cough since 1 month, productive with scanty sputum, which was white in colour, non blood tinged, non foul smelling, aggravated on exertion and exposure to cold weather and relieved with medication. It was associated with cold
She also had shortness of breath since 2 days, grade 2, which was aggravated on exertion and relieved by taking rest and medication, no orthopnea, no PND.
She complained of burning sensation in the oral cavity since 3 days
No h/o hemoptysis, chest pain, loss of weight.
Daily Routine:
Before she got ill, she used to wake up at 8am every morning, following which she would cook, wash the dishes, clean the house and boil water to take a bath, then she would take a bath by 10am and have breakfast of rice and curry. (??)
Past History:
She had similar complaints 2 years ago which was treated by unspecified medications.
k/c/o asthma since 30 years, on formoterol and budesonide (metered dose inhaler)
she has complaints of left sided neck pain 3 years ago, dragging type, radiating to back and left shoulder, aggravated on exertion, not relieved by medication, associated with giddiness and vomiting.
diagnosed with type 2 diabetes two weeks back
not a k/c/o HTN, CAD, TB, epilepsy, thyroid disorders.
Surgical History: no surgical history
Family History: no significant family history
Drug History: formoterol and budesonide (metered dose inhaler)
General Examination:
I have examined the patient after taking prior consent and informing the patient in the presence of a female attendant. The examination was done in both supine and sitting position in a well lit room.
- patient was conscious, coherent and cooperative
- well oriented to time and space
- well built and adequately nourished
- pallor present
- no icterus
- no cyanosis
- clubbing of fingers present
- no lymphadenopathy
- no pedal edema
- no malnutrition
- no dehydration


Vitals:
- temperature: 97.3 C
- pulse: 96 bpm
- respiratory rate: 22 cycles/min
- BP: 130/90 mm of Hg

Fluid Intake and Urine Output
Total Input: ml
Total Output: ml
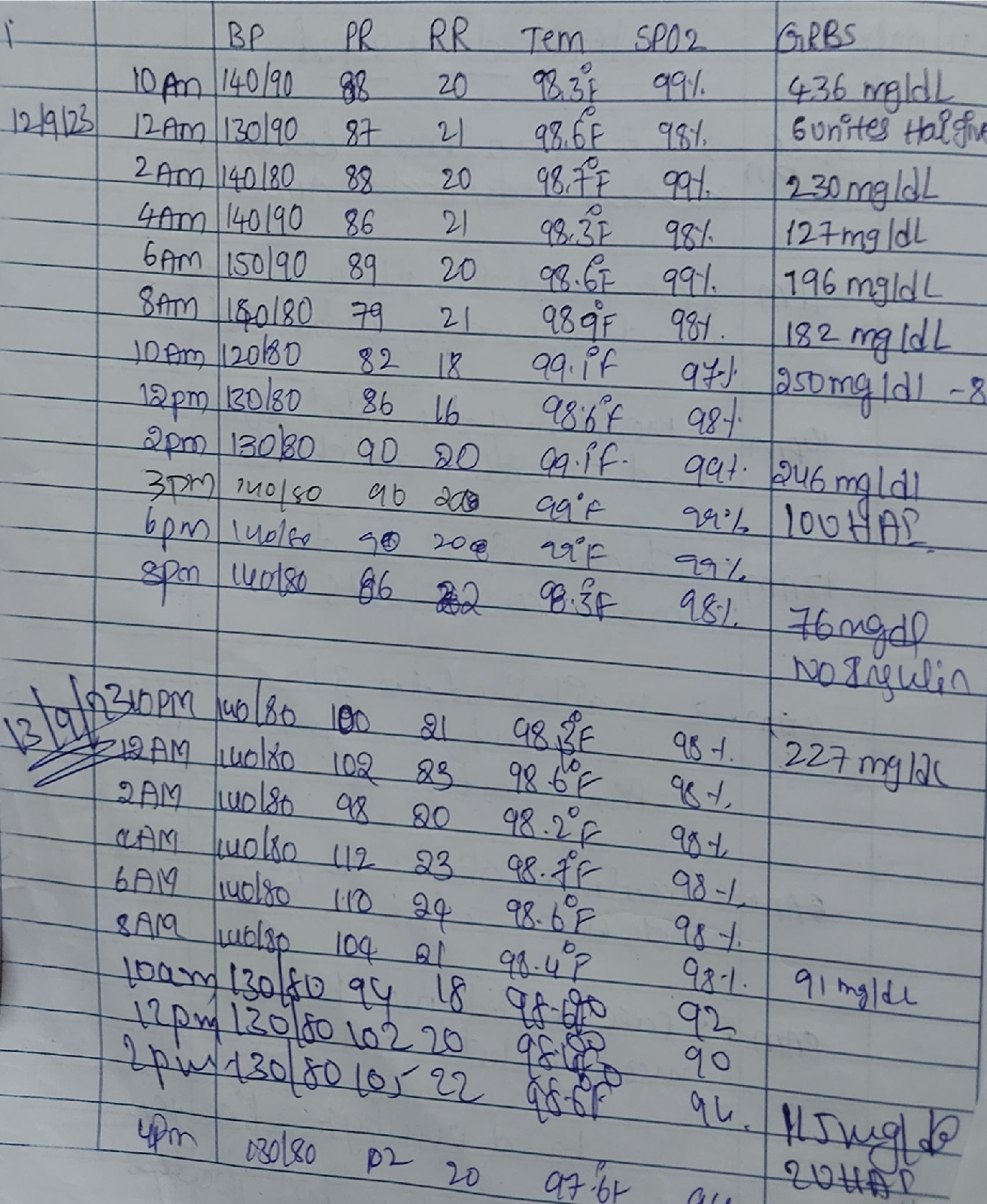
Fever Chart: (as above)
Systemic Examination:
RESPIRATORY SYSTEM
Patient examined in sitting position
Inspection:
- Upper respiratory tract - nose & oropharynx appear normal. Oral cavity - few ill defined white colour plaques over buccal mucosa and soft palate.
-Chest appears bilaterally symmetrical & elliptical in shape
- dyspnea present
-Respiratory movements appear equal on both sides and it's thoracoabdominal type
-Trachea central in position & Nipples are in 5th intercoastal space
-No dilated veins, sinuses, visible pulsations.
Palpation:
-All inspiratory findings confirmed
-Trachea central in position
Percussion:
Dull note
Auscultation:
-Supraclavicular- (NVBS) (NVBS)
-Infraclavicular- B/L rhonchi
-Supramammary- B/L rhonchi, crepts
-Inframammary- B/L rhonchi, crepts
-Axillary- B/L rhonchi,
-Infra axillary- B/L rhonchi, crepts
-Suprascapular- B/L rhonchi, crepts
-Interscapular- B/L rhonchi
-Infrascapular- B/L rhonchi, crepts
CARDIOVASCULAR SYSTEM
Inspection :
-Shape of chest: elliptical
-No engorged veins, scars, visible pulsations
Palpation :
-Apex beat can be palpable in 5th intercostal space
- no cardiac thrills
Auscultation :
- S1, S2 are heard
- no murmurs
ABDOMEN
- shape: obese
- no tenderness
- no palpable mass
- no bruits
- no free fluid
- hernias orifices: normal
- liver: not palpable
- spleen : not palpable
- bowel sounds heard
- genitals:
- speculum examination :
- P/R examination :
CENTRAL NERVOUS SYSTEM
- conscious
- normal speech
- no neck stiffness
- no Kerning's sign
- cranial nerves: normal
- sensory : normal
- motor: normal
- reflexes: all present bilaterally
- finger nose in coordination: no
- knee heel in coordination: no
- gait: normal
Investigations:
12/09/2023:










Provisional Diagnosis:
-acute exacerbation of asthma
- stage 3a CKD
- de novo type 2 DM
- hypokalemia secondary to urine loss
- oral candidiasis
- k/c/o asthma since 30 years