Hi, I am Manasvi Peddineni, 5th sem medical student. This is an online E-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
CONSENT AND DE-IDENTIFICATION :
The patient and the attenders have been adequately informed about this documentation and privacy of the patient is being entirely conserved. No identifiers shall be revealed throughout this piece of work whatsoever.
Chief Complaint: A 34 year old male, resident of Ramanapet, painter by occupation, came to the OPD with chief complaint of
- pain abdomen since 4 days.
History of Presenting Illness: Patient was apparently asymptomatic 6 years ago when he developed pain Abdomen, for which he visited a local physician and was prescribed unspecified medication. The pain subsided upon using this medication.
-2 years ago he had same complaints and visited KIMS and the pain subsided after using the prescribed medication.
- 4 days ago he developed pain abdomen in the epigastric region, colicky type, radiating to the back, aggravated by food and water intake, relieved by bending forward.
- it was also associated with single episode of projectile vomiting, which was non bilious and had water as its content.
- h/o consumption of alcohol 4 days ago
- no h/o trauma, fever, diarrhea, constipation, malena, cough, SOB, burning micturition, reduced urine output.
Daily Routine:
-Before he got sick (4 days ago), he used to wake up at 6:30am, eat rice for breakfast and go to work as a painter. At 1pm he used to have lunch (rice) at work. He used to complete his work and come back home at around 6:30 - 7pm. He usually had dinner (rice) at 8pm and then went to sleep.
-After he got sick (since 4 days), he wakes up at random times between 5 am to 9 am, has meals when given by attender and lies in bed most of the time.
Past History: he had similar complaints 6 years ago, and 2 years ago.
not a k/c/o DM, HTN, CAD, TB, asthma, epilepsy, thyroid disorders.
Surgical History: no previous surgical history
Family History: not significant
Drug History: unspecified medications taken in the past to relieve abdominal pain
General Examination:
I have examined the patient after taking prior consent and informing the patient in the presence of a female attendant. The examination was done in both supine and sitting position in a well lit room.
- patient was conscious, coherent and cooperative
- well oriented to time and space
- well built and adequately nourished
- no pallor
- no icterus
- no cyanosis
- no clubbing of fingers
- no lymphadenopathy
- no pedal edema
- no malnutrition
- no dehydration


Vitals:
temperature: afebrile
PR: 86 bpm
RR: 18 cycles/min
BP: 120/90 mm of Hg
Fluid Intake and Urine Output
Total Input: ml
Total Output: ml
Fever Chart:
Systemic Examination:
CARDIOVASCULAR SYSTEM
Inspection :
-Shape of chest: elliptical
-No engorged veins, scars, visible pulsations
Palpation :
-Apex beat can be palpable in 5th intercostal space
- no cardiac thrills
Auscultation :
- S1,S2 are heard
- no murmurs
RESPIRATORY SYSTEM
Patient examined in sitting position
Inspection:
- Upper respiratory tract - oral cavity, nose & oropharynx appear normal.
-Chest appears Bilaterally symmetrical & elliptical in shape
- dyspnea if present
-Respiratory movements appear equal on both sides and it's abdominothoracic type (males).
-Trachea central in position & Nipples are in 5th Intercoastal space
-No dilated veins,sinuses, visible pulsations.
Palpation:
-All inspiratory findings confirmed
-Trachea central in position
Percussion:
Resonant
Auscultation:
-Supraclavicular- (NVBS) (NVBS)
-Infraclavicular- (NVBS) (NVBS)
-Supramammary- (NVBS) (NVBS)
-Inframammary- (NVBS) (NVBS)
-Axillary- (NVBS) (NVBS)
-Infra axillary-(NVBS) (NVBS)
-Suprascapular- (NVBS) (NVBS)
-Interscapular- (NVBS)
-Infrascapular- (NVBS)(NVBS)
ABDOMEN
- shape: scaphoid
- tenderness present in epigastric region
- no palpable mass
- no bruits
- no free fluid
- hernias orifices: normal
- liver: not palpable
- spleen : not palpable
- bowel sounds heard
- genitals:
- speculum examination :
- P/R examination :
CENTRAL NERVOUS SYSTEM
- conscious
- normal speech
- no neck stiffness
- no Kerning's sign
- cranial nerves: normal
- sensory : normal
- motor: normal
- reflexes: all present bilaterally
- finger nose in coordination: no
- knee heel in coordination: no
- gait: normal
Investigations:
Hemogram:


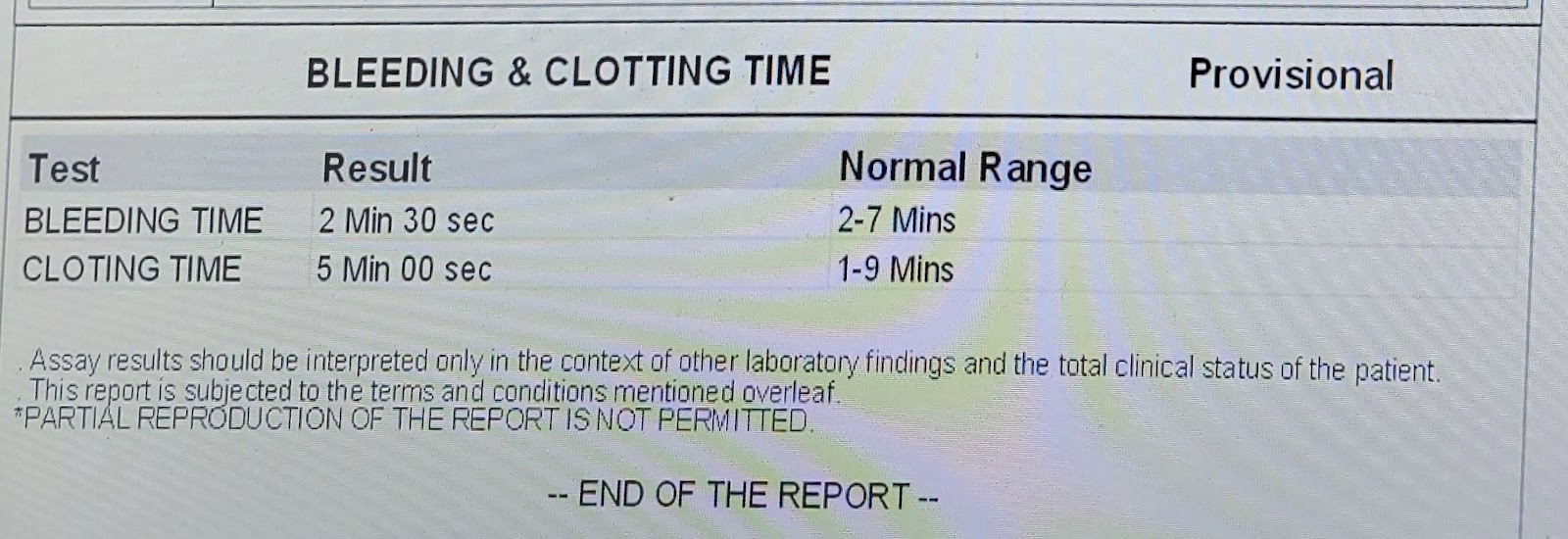
Bleeding and Clotting time:
Activated partial thromboplastin time:

Serum magnesium:

Serum electrolytes:

Blood urea:

Serum creatinine:

Lipase:

Serum amylase:

Provisional Diagnosis: ACUTE PANCREATITIS
Treatment:
INJ. tramadol I.V
INJ. Pantop 40mg I.V
INJ. Zofer 4 mg I.V
I.V Fluids